

Glaucoma is like pushing on a basketball
 We learned a ton of stuff about the eye on today’s Healthy Matters broadcast. We mostly focused on glaucoma (good pun, eh. . . see how I said focused while talking about vision . . . oh never mind). We also touched on macular degeneration, cataract, and other topics raised by listeners.
We learned a ton of stuff about the eye on today’s Healthy Matters broadcast. We mostly focused on glaucoma (good pun, eh. . . see how I said focused while talking about vision . . . oh never mind). We also touched on macular degeneration, cataract, and other topics raised by listeners.
My guest was HCMC ophthalmologist Anne Abel. If you missed the show, be sure to click here to listen to the podcast. She’s a terrific teacher and explains the complexities of the eye really well. That’s her in the picture, giving out serious advice while I distract her by taking pictures!

For instance, here is what we learned today:
- Checking for glaucoma is like pressing your hand on a basketball.
- The lens of the eye is like an M&M.
- Eye doctors drain the fluid from your eye just like a plumber clears a drain.
- The cornea is the windshield of the eye.
That’s all there is to it. Nothing too complicated here. So Dr. Abel is a great surgeon AND she explains things as complex as the eye in a way people can understand. Geez I wish they had taught it that way in medical school!
I’ll touch on a few of the topics we covered on the show today, including M&Ms, basketballs, clogged drains, and windshields – and then I’ll wrap up with some responses to text messages we didn’t get to cover on the broadcast. Read on.
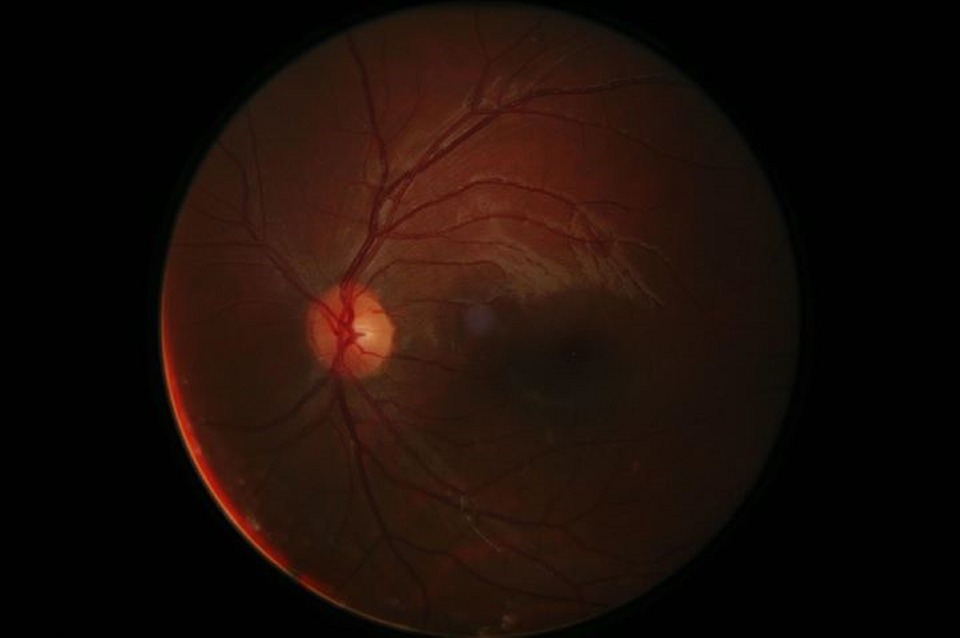
The Mars-like picture above is the back of your eye as seen by your doctor. The bright spot is the optic nerve (literally a portion of your brain visible to the unaided eye) and the lines are blood vessels. Tell me this isn’t cool.
Glaucoma
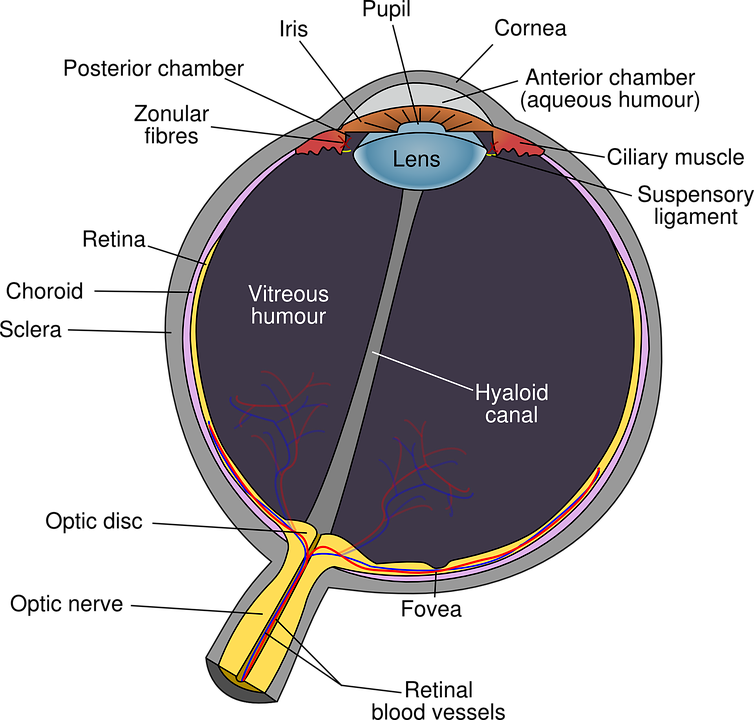
Dr. Abel’s basketball metaphor is apt. Your eyeball really is like a basketball – only it isn’t filled with air but rather with a gelatinous gooey mass called vitreous humour in the back part and the liquid aqueous humour in the front part. The vitreous comes from the Latin vitrum which means glass and it stays relatively unchanged throughout life. I guess it is shiny and translucent like glass – hence the name. You are born with it and it may serve to keep the structure of the eye intact, but interestingly, an eye doctor can surgically remove it and you will do fine.
The aqueous humour (aqueous coming from the Latin for water) is a different story. This fluid is continuously produced and circulated around the front part of your eye and serves to keep the pressure at the right level. Too much pressure in the eye over time can damage the critical optic nerve which carries visual signals to your brain. Damage the optic nerve and vision loss may result. This is the condition called glaucoma, and it is a leading cause of blindness so it is a big deal. I should mention here, as did Dr. Abel on the radio show, that not all glaucoma fits this neat definition as there are several types and one of them does not feature increased pressure in the eye. So there you go.
For the most part, though, just like pushing on a basketball to check the pressure, your eye doctor is checking the pressure in your eye when testing for glaucoma.
A couple other facts about glaucoma:
- It comes on slowly and is usually painless, so you don’t realize you have it.
- Your peripheral vision (out to the sides) is often affected first, so you may be compensating for that by glancing side-to-side without even knowing it.
- Testing is easy and also painless (they numb the eye surface before testing).
- Treatments exist and they work, but any existing damage to the all-important optic nerve that has already occurred can’t be reversed. Drops can lower eye pressure either by reducing production of the aqueous or by making it easier to drain what fluid is there.
- Laser treatments and surgery are also effective when the drops are not enough – hence the plumber and the drain metaphor (if you don’t know what I’m talking about – listen to the podcast! for more on plumbing and the eye).
For more information on glaucoma, you may want to check out the Glaucoma Research Foundation at glaucoma.org.
Cataract
This is where M&M candy comes in handy. Imagine the lens of your eye, which Dr. Abel tells us is rather like an M&M, presumably not the peanut kind. This structure just inside the opening to your eye helps to focus the image on your retina. Trouble is, as we age the lens gets cloudy, a condition known as cataract. The word itself comes from the Greek for waterfall so I’ve kindly included a picture of a cataract for you. Oops, wrong kind of cataract but it does beg the question about why the eye condition is from the same word as a waterfall. I will leave it to your imagination.
F ortunately, this one is a cinch for an ophthalmologist to fix with a simple surgery. Now it always sounds somewhat disconcerting to me when the procedure is described, but really it is an effective, common, and safe procedure. The lens is simply broken up and removed and a new, synthetic one is implanted.
ortunately, this one is a cinch for an ophthalmologist to fix with a simple surgery. Now it always sounds somewhat disconcerting to me when the procedure is described, but really it is an effective, common, and safe procedure. The lens is simply broken up and removed and a new, synthetic one is implanted.
As we talked about on the air, many people barely even know what they have been missing since cataract, like glaucoma, is slow to develop and is painless. It is easy to diagnose and treat, however, so if your vision isn’t all it used to be and you have reached, ahem, a “certain age” then by all means have a doctor take a peek. You’ll be glad you did.
Cornea – the windshield of the eye
I’m often stymied when trying to describe the cornea – I’m usually fumbling around trying to come up with a good description which ends up something like “the cornea is the clear part overlying the iris, sort of covering up the color part of your eye and it keeps stuff out of the eye” or some such verbiage. On the show today, Dr. Abel was much better at it – the cornea is like the windshield of your eye. Gotta give her credit, that about sums it up without much more elaboration.
Being a clear windshield-like thing, finding a decent picture of just the cornea proved to be too much for my capabilities, so here’s a picture of a regular human eye. Imagine the windshield over those baby blues and that’s the cornea.
The topic of the cornea came up when a caller asked about pain following a cornea transplant. Too much to get into on this blog post, but cornea transplant (aka keratoplasty) is safe and successful in the vast majority of the cases. It is usually done when your own cornea is damaged due to trauma, infection, previous surgery, and the like and happily the supply (from deceased donors) is usually adequate.
Which brings me to some unanswered texts from the Healthy Matters mailbag. If you are new to the blog . . . I get many texts and phone calls to the live radio broadcast each week – too many to handle on the air. So I try to answer a few every now and then on this blog. Nothing in depth, just a little bit of info for each.
One Healthy Matters listener asked: “What is Fuchs’ dystrophy?”
Pronounced fooks dystrophy, this is a condition in which fluid builds up in your cornea (the windshield) and leads to thickening of the cornea, resulting in blurry vision, sensitivity to light, perhaps a glare overlying the vision. It is more common in women, people over 50, and may be inherited. Treatment usually starts with eyedrops to relieve the swelling but surgery may be needed and is usually quite successful.
Another listener asked if we could “talk about macular degeneration.”
I really wanted to say much more about this condition, as macular degeneration is so common and I don’t get to have an ophthalmologist like Dr. Abel on all that often. She did talk about wet and dry macular degeneration a bit on the air, but since time was short we didn’t get into it in much detail. I think I’ll ask her back for a more in-depth conversation on a future show.
Basically, dry macular degeneration is a thinning of the macula (the part of your retina responsible for seeing straight ahead – your central vision). Compare this to glaucoma in which the peripheral vision usually is affected first. There is no terrific cure for dry macular degeneration, but eye vitamins (like lutein) may help.
The less common wet macular degeneration may come on a bit faster than the slower onset dry type. The wet form is due to overgrowth of blood vessels under the central retina.
Again, macular degeneration is too big a topic for now. Look for a whole radio show on it in the future.
As someone who has a few eye problems of my own – I’ve had surgery at age 3 for lazy eye, I’m basically color-challenged (color-blind, anyone?), and the astigmatism in my left eye means the lens in my eyeglasses on that side is awfully thick – I really appreciate the magnificence of the eye. I hope you’ve learned a bit from the show today and/or this blog post.
 I want to thank Dr. Anne Abel for helping us out on our eye show this morning. To see her or any of my awesome colleagues at HCMC, the number is 612-873-6963 or go to hcmc.org. And as always, please leave me a comment below if you have a question, an idea for a future radio show topic, or you just have something to say!
I want to thank Dr. Anne Abel for helping us out on our eye show this morning. To see her or any of my awesome colleagues at HCMC, the number is 612-873-6963 or go to hcmc.org. And as always, please leave me a comment below if you have a question, an idea for a future radio show topic, or you just have something to say!
When Breath Becomes Air – Healthy Matters Book Club
“I began to realize that coming in such close contact with my own mortality had changed both nothing and everything.”
Paul Kalanithi, from When Life Becomes Air
Welcome to Healthy Matters Book Club! This is the first of what I hope will be many posts in which I will explore a health & medicine book that I have read and found interesting . I’m not a book critic and this is not a thorough book review – just a couple of my thoughts. I hope you will read it and join the conversation by leaving a comment below or perhaps joining me on Twitter @DrDavidHilden. Plus, I’m hoping you will leave me book discussion suggestions in the comments – I’m always looking for a good read!
Today’s Book: When Breath Becomes Air
Re-read the quote at the top of this post. It is a pretty good summary of When Breath Becomes Air, the recent book from Dr. Paul Kalanithi. I strongly recommend the book to you – it is a quick read – just a few hours – but it is gripping.
Dr. Kalanithi died in March 2015 and the book is a memoir of his last months of life. An accomplished neurosurgeon and a rising star in the medical community, Paul Kalanithi learned of a terminal diagnosis when he was just 35 years old. Also a talented writer who was initially torn between a career in medicine or as a writer, he set out to chronicle his life knowing that he would not live a great deal longer. He is a terrific writer and his prose is quite lyrical – almost poetic to the degree that some may find a bit much – and I found it brilliant.
Paul writes with an intimacy rarely seen in books by doctors. Neurosurgeons, fairly or not, are not known for their sensitive sides. But in this case, the surgeon becomes the patient and is faced with what he knows in his mind and in his gut – that he has a disease from which he will certainly die. He knew it the instant he looked at his own CT scan. This unnerved me a bit as I can imagine any of my colleagues facing the same situation in which we look at our own medical results and know a bit too much what it means for us.
When I was reading the book, I couldn’t escape the knowledge that the writer has already died and is really speaking from the grave. Made me pause more than once or twice.
But it is a great read even if you are not a doctor. Maybe even more so, as it gives you an unfiltered glimpse into the mind of a brain surgeon with a soft spot for poetry. You really feel like you get to know him. And just as great is that you get to meet Lucy, his wife, who seems to me an incredible person.
Throughout the reading I couldn’t escape the knowledge that Lucy and their infant daughter are still here – real people, alive and carrying on their lives. To me Lucy is as fascinating as her husband and her epilogue is as poignant as her husband’s writing. Now about one year after his death, she has found herself doing something she probably didn’t imagine just 2-3 years ago – she’s on a book tour for her late husband.
Here’s an interview she did on National Public Radio that I encourage you to listen to:
“Live as if you were to die tomorrow. Learn as if you were to live forever.”
This oft-quoted bit of wisdom by Gandhi was realized by Dr. Kalanithi during his lifetime. After his awful diagnosis, he continued to practice surgery, continued to read, continued to write, continued to love, continued to learn, and continued to reflect on what is important in life. He indeed was acting as if he may well live forever.
But he also acted as if he may die tomorrow which for him was not an abstract concept but a real possibility. One aspect of their lives that gets my thoughts all tied up in knots is their decision to have a baby, knowing that he would not live to see their child grow up. Here is an exchange from the book:
“Will having a newborn distract from the time we have together?” she asked. “Don’t you think saying goodbye to your child will make your death more painful?”
“Wouldn’t it be great if it did?” I said. Lucy and I both felt that life wasn’t about avoiding suffering.”
Can you imagine having such a conversation when thinking about having a child? Holy cow. Listen to the audio clip above to hear Lucy say more about this.
Join the discussion!
What would you do if you knew you had a very limited amount of time to live? Would you continue to work at whatever you do? Would you drop everything and try something new? What would you do if you were Lucy – his spouse? Are you a “live-for-the-moment” type or a “planner for the future” type? Maybe a little of both?
So now it’s your turn. Read the book and leave a comment below with your reactions. I’d love to hear your thoughts!
Also, if you have read a health/wellness/medical book that you’d like to recommend – leave me a comment right here on the blog (in the comments section below). Can be fiction or non-fiction. Maybe we can discuss it on a future post on the Healthy Matters Book Club!
![]()
![]()
![]()
![]()
![]()
![]()
No more ipecac! National Poison Prevention Week 2016
I have the great fortune to work side by side with the smart folks at the Minnesota Poison Control Center, which is housed right here in my hospital. Each year we try to do a service to the community by hig hlighting National Poison Prevention week, which is going on right now. Dr. Jon Cole is the Medical Director of the Poison Center, and Kirk Hughes is the Education Director. You won’t find two more dedicated experts than these two guys – and I was happy to have them on the Healthy Matters broadcast this week. That’s Dr. Cole’s smiling face on the left and Kirk below – bright and early on a Sunday morning. Now wouldn’t you want this guy to be the one helping you?
hlighting National Poison Prevention week, which is going on right now. Dr. Jon Cole is the Medical Director of the Poison Center, and Kirk Hughes is the Education Director. You won’t find two more dedicated experts than these two guys – and I was happy to have them on the Healthy Matters broadcast this week. That’s Dr. Cole’s smiling face on the left and Kirk below – bright and early on a Sunday morning. Now wouldn’t you want this guy to be the one helping you?
Listen to the podcast of the show here by clicking the logo here –> .![]()
I encourage you to click the link to the Minnesota Poison Center. It is a site loaded with information, including tip sheets that you can download for your own use.
My own daughter and the iron tablets
First my personal tale of woe. I mentioned on the radio show about a brush with poisoning with our own daughter. The story is a scary one for any parent . . . our little one was just 1 or 2 years old when we found her on the floor with an open bottle of iron tablets, some of them spilled out. We had no idea if she had swallowed any of them. Yikes. Iron tablets don’t sound all that bad, right? But these common supplements are really dangerous in overdose for the wee ones. So we took her to a doctor and she had to have a x-ray (to look for the pills in her digestive system). Thankfully she was all right, but today we would have called 1-800-222-1222 and talked to the poison experts.
What I learned about poison prevention
Here are just a few of the things our listeners learned from Dr. Cole and Kirk (that’s Kirk in the picture below – he’s a guy with a head-full of knowledge from his career as a nurse, a basic EMT, and a poison prevention educator). And down below, look for a neat video of Kirk in action with a grateful parent. It’s worth a few minutes.
- The most important thing of all – know this number. 1-800-222-1222. This is the number for the Poison Center, and the beauty of it is that it is valid nationwide. The system will direct your call to the Poison Center nearest you, based on th
 e area code you are calling from (or the area code of your cell phone).
e area code you are calling from (or the area code of your cell phone). - Calling the Poison Center number is the first thing you should do if you have a question about poisoning – unless you or a child is experiencing chest pain, difficulty breathing, or seizures. In that case, call 911.
- It doesn’t have to be an emergency – call if you simply have a question.
- In the vast majority of cases (>90% of the time), the experts at the Poison Center can safely get you advice and treatment recommendations while you stay at home. It is highly likely that you can avoid a trip to the Emergency Department or clinic by calling them first.
- Program the number into your cell phone under Poison Center!
A word about keeping kids safe
More than half the calls to Poison Centers involve children under the age of six, and the problems are usually right in their own homes. Kirk and Dr. Cole told us that there are several reasons why kids are at risk in the home. Could these happen at your house?
- Poisons are not stored properly. Keep them up high, in original containers, well out of reach of curious minds. Grandparents, your home may have your pills out on the counter or bathroom sink where you won’t forget them. But if little ones come to visit, it takes just a second for them to grab them and swallow them. Keep your grandchildren safe by keeping the medications out of sight!
- Children are naturally curious. Pills look like candy. Spray bottles look interesting. Brightly colored liquids look pretty. But all can be deadly.
- Many poisonous liquids look and smell like something safe to drink. Fuels, cough syrups, even shampoo are like this. Keep them out of sight and not accessible to kids.
- Children imitate adults. They see you taking medications or drinking liquids, they are certain to try to do the same.
This all sounds like common sense but in reality, many if not most of our homes are not particularly safe for children. So if you have kids coming to visit, think of how to keep them safe. It just takes a second when you are not paying attention for a kid to get into something that is really dangerous to them. In my little story of my daughter’s scare with iron tablets, we failed to do these simple things. Now I know better!
What about good ‘ol syrup of ipecac?
Lots of us probably still have an old crusty bottle of syrup of ipecac in our cabinets, especially if you are a bit older. Well get rid of it! It is no longer recommended to use ipecac to get kids or adults to vomit. If fact, you should not even keep it in your home. Ipecac is yesterday’s news. Today, call 1-800-222-1222 instead.
Final thoughts
Poison prevention is a huge topic that I could never cover in a blog post such as this. Rather, I hope to have provoked you to think a little bit more about keeping ourselves and our kids safe.
A listener to our Poison Prevention show on Healthy Matters posed the simple but really good question – just what is considered a poison? I learned that a poison can be darn near anything – medications, cleaning supplies, fumes in the air, plants in your garden. I also learned that poisoning is the leading cause of injury death in the United States.
Here’s that video of Kirk Hughes in action, about a family far away from a hospital but who did the right thing and called the Poison Center:
A final word on the Poison Control system in the United States. Poison Centers are available to you:
- Anytime. 24/7, including holidays
- Anywhere. Call from home, school, business. Anywhere in the country.
- Anyone. Whether you are a concerned parent, a caregiver, a senior, a teenager, a teacher, a clinician – experts are there to help you.
And it comes free of charge to you.
1-800-222-1222. It’s a number you should know.