

The one where I get a colonoscopy
 See that brave patient in the picture? Yup, that’s me, just minutes from getting my colonoscopy at HCMC last year. I’ve been meaning to do a post about that experience and now seems as good a time as any. What with turmoil in the country and all, what could be better than to re-live the day somebody put a 5-foot long tube inside me to have a peek?
See that brave patient in the picture? Yup, that’s me, just minutes from getting my colonoscopy at HCMC last year. I’ve been meaning to do a post about that experience and now seems as good a time as any. What with turmoil in the country and all, what could be better than to re-live the day somebody put a 5-foot long tube inside me to have a peek?
It must be on lots of minds if last week’s radio broadcast was any indication. The phone and text and Twitter (@DrDavidHilden) lines were full of questions about colon cancer and how to avoid it.
Here’s the podcast of that show for you to listen to if you missed it (Healthy Matters show #420 – 1/22/2017)
I like to have a little fun with most medical topics, and I gotta say that if there ever was a medical topic worthy of humor, it has to be getting a colonoscopy. I mean, really, think about it. It has all the ingredients of a comedy routine:
- Gross part of the human anatomy. Check.
- Flushing out the entire contents of your intestines. Check.
- Baring your rear end to complete strangers while lying curled up on your side wishing you were literally anyplace else at that moment. Check.
- Complete surrender of any sense of dignity you had walking in the door. Check.
- Passing gas all day when it is over. Check.
What could be more fun?
But colorectal cancer really is no joke. In this post, I hope to accomplish three things:
- Convince you that getting screened for colorectal cancer makes sense.
- Introduce you to the various ways you can get screened.
- Allay any anxiety you may have over the whole subject.
Colorectal cancer: the bad news
In all seriousness, getting a screening test for colon cancer is among the most effective things you can do for your health. In fact, amid all the unpleasantries people endure in an effort to stay healthy, this one ranks way up there in importance. So let me repeat, getting screened for colon cancer is important and potentially lifesaving.
Check out the sobering news on colorectal cancer:
- It is common. Colorectal cancer is the 3rd most common cancer in men and women (skin cancers excluded).
- It can be deadly. Colorectal cancer is the second most common cause of cancer death in men (behind lung cancer), and the third most common cause of cancer death in women (behind lung and breast cancer).
- It is potentially treatable (and dare I say?), curable. Check this fact out – for those whose colorectal cancer is caught early, fully 90% will likely still be alive in 5 years. But for those with advanced cancer, only 15% will still be alive in 5 years.
A quick plug for some of the best medical information on the Internet. It comes from the Centers for Disease Control. For more on colon cancer from the CDC, click here.
It is largely because of that last bullet point that you should get screened for colorectal cancer. There is a dramatic difference in your chances of survival if you can only catch the cancer early on. That is true for most cancers, but it is especially true with this one.
This is a good time to point you toward the American Cancer Society’s Cancer Statistics Center. If you are curious about colorectal or any other cancer statistics, it is a great site to check out. You can sort the stats by your state of residence or type of cancer. It’s cool.
Ways to get screened
Hopefully I’ve convinced you of the importance of getting screened. Or maybe you didn’t need convincing in the first place! Let’s turn now to the various ways you can get the job done.
What you may not know is there are several ways to get your colon checked out. The one we all know and love is the colonoscopy but you may not know that it is not the only way to go. That surprises some people when I tell them that. There is a misconception floating around that the “best” way to go is the colonoscopy and that all the other methods are inferior. Not so, not so. It is the test of choice for many people (it is what I did) but it isn’t for everybody. And if the thought of an invasive procedure leads you to proscratinate forever in getting it, you are not getting the benefit of the test anyway.
As a wise person once said, “The best test for colon cancer screening is the one that the patient will actually do.”
So let’s look at the various tests you can consider:
FOBT and FIT tests
These are the tests in which you submit a little tiny stool sample and the test looks for blood in your stool that you can’t even see (hence the word “occult”). They are similar in that you usually can collect the sample at home, they are not invasive, and they are pretty good at finding hidden blood. They work under the principle that cancers and the pre-cancerous polyps in the colon tend to bleed.
FOBT stands for Fecal Occult Blood Test and sometimes has a little “g” in front of it (g = guaiac, so it looks like gFOBT). It’s the older one of the two and we’re seeing it used quite a bit less today. I think it will fade into oblivion . . . in favor of . . . FIT testing.
FIT stands for Fecal Immunochemical Test (sometimes written iFOBT with the little “i” = immunochemical). It is newer and uses a fancier approach to detecting blood proteins. It has the same advantages as the gFOBT but it has additional advantages over gFOBT in that it is probably more accurate and no dietary restrictions are needed prior to doing the test. Here’s a bit more on the FIT test.
Both of these stool tests need to be done every year. And if they find blood in your stool, you may need a colonoscopy after all! But they are a good choice for many people.
FIT-DNA
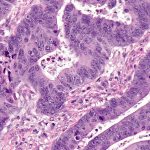
Photo: Nephron via Wikimedia Commons
This is the newest of the bunch. It works in a similar way to the FIT test above, but rather than look for blood, it looks for abnormal DNA in your stool. In other words, it is looking for the genetic “fingerprint” of cancer cells. Pretty cool, high-tech stuff here! The picture at left, though not of the DNA itself, is a biopsy specimen showing colon cancer cells. They are the angry looking cells throughout this piece of tissue.
This test needs to be done every three years but the data is not too certain on this yet since it is so new. It also may not be covered by your insurance. It is really promising though! We will be seeing a lot more of this one in the future, I think.
Flexible sigmoidoscopy
I’m not seeing too much of this method lately. It is sort of like a “mini-colonoscopy” in that a camera on a flexible tube is inserted into the colon. It doesn’t require the extensive colon flush, doesn’t need as much sedation, and complication rates are lower. Since it only looks at the lower part of the colon, however, it can miss any cancers that are higher up.
This test needs to be done every 5 years and lots of people get the stool tests in addition to it.
Colonoscopy
This is the one most of us think about. A specially trained doctor (a gastroenterologist – basically a really talented person with an inexplicable tolerance for looking at the nether regions of people) inserts a long-flexible camera into your intestines, all the way to the point where your large intestine (your “colon”) begins. Which is about 5 feet up there. Believe me, they are able to get a good look and simply see with their own eyes if you have a lesion (cancer or polyp). The advantage is that if they see something bad, they can either remove it entirely (like a polyp) or take a biopsy (to see if it is a cancer).
Cool picture time. Here’s a normal intestine as seen by your gastroenterologist (this one is actually in the rectum):

Photo: Melvil via Wikimedia Commons
Here’s an intestine with a polyp (don’t know if it is the pre-cancerous kind or not, but that’s why we take them out!)
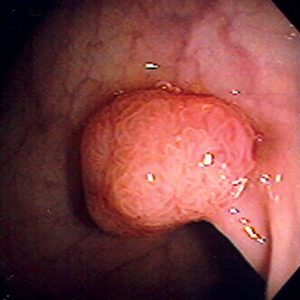
The other advantage is that for most people, colonoscopy only needs to be done every 10 years, perhaps every 5 years if they see something concerning.
But there are disadvantages to the colonoscopy. There is a small, but real, risk of perforation, which is where the colon wall gets a hole in it. And this is bad. Remember, your colon is full of bacteria and other unpleasantness. The outside of your colon (in your abdominal cavity) is sterile. You really don’t want the contents of your intestines to spew out into your belly. That can lead to a condition called peritonitis which can lead to sepsis which can be very serious.
Fortunately, this is a rare complication (estimates range from 1 in 500 all the way down to 1 in 6000). And although big perforations usually require surgery right away, many small perforations can heal themselves.
Virtual colonoscopy
I feel like I should mention this one (technically called CT colonography). It uses x-rays (a CT scan) to look at the colon non-invasively. Super tempting to go this route as it eliminates the invasiveness and thus the risk of colonoscopy. But I don’t see too many people getting the virtual test done. After all, it does expose you to radiation (albeit not a whole lot), and if it finds something abnormal, you still have to get the colonoscopy anyway.
My colonoscopy
I’ll end with my own story. I figure doctors who are counseling patients to get tested better be doing it for themselves, eh?
So I turned the magic age of 50 a while back and for most people, that is the age where all this colon talk gets real, real fast. I’m talking people at average risk. Others at higher risk (say your dad had cancer at an early age, for example) should do it sooner.
So I decided to go for it on a winter day last year. I saw my doctor (yup, I actually have a doctor that I see, though I have to admit it was turning 50 that prompted me to finally get a doctor of my own. Tsk-tsk, I know). He prescribed all the prep stuff which I faithfully did.
 Have you ever done the colon prep? Many of you remember getting such a large volume of the prep solution that you practically needed a grocery cart to get it home. You’d go to the pharmacy to pick it up, and they would push to you across the counter like a zillion gallons of the stuff in big jugs. You’d swear there was a mistake, that you were only getting the prep for one person not the whole family. But it was real. That was the way we used to do it (and still do for some people as it does actually work). You drank the solution the night before the colonoscopy until it came out the bottom end looking just like it did going in the top end – like clear water.
Have you ever done the colon prep? Many of you remember getting such a large volume of the prep solution that you practically needed a grocery cart to get it home. You’d go to the pharmacy to pick it up, and they would push to you across the counter like a zillion gallons of the stuff in big jugs. You’d swear there was a mistake, that you were only getting the prep for one person not the whole family. But it was real. That was the way we used to do it (and still do for some people as it does actually work). You drank the solution the night before the colonoscopy until it came out the bottom end looking just like it did going in the top end – like clear water.
My prep was of the newer kind. Instead of gallons of prep solution, I went the route where you pour an entire bottle of a laxative powder into a bottle of sports drinks and drink it down in a few sittings. Then you wait for the action to begin. And you spend most of the next 12-24 hours in the bathroom. This is a good time to get a supply of reading material and to tell your family to clear out of the place – for their own good.
Sometimes I think the people who devise these prep schemes are deranged.
So I did all that the night before my test. Then I show up for my colonoscopy to the GI Lab at HCMC, which is the hospital where I work. A couple points about that. First, why do they have to call it the GI Lab? Are they doing experiments in there? Second, it does take a bit of self-assurance to get your colonoscopy at your own workplace. I’m sitting there in a hospital gown with my rear end exposed for all the world to see when 2 or 3 people I see in the hallways all the time come in. Tough to maintain any sense of workplace decorum in that situation, I think.
So being the talker that I am, I try to make small talk with the nurse whom I know I will see a few hours later in the cafeteria line. He’s all professionalism, thankfully. And the doctor comes in, but I don’t make much eye contact with her, my backside being the side of interest, after all.
I assure the team that I will be watching my entire colonoscopy on the video monitor, just like Katie Couric did on live television a few years ago. And I really intended to watch because I was genuinely curious to take a gander at my own intestines from the inside out. That’s actually a pretty cool opportunity when you think about it. I thought I did a pretty good job staying awake. But then at one point I looked at the screen only to find out that the doctor was just finishing the whole procedure. She had done my entire colonoscopy and I dozed off for the whole of it!
I went home, had an uneventful day and made it to work the next day as good as new.
My point being: this was no big deal. To prove it, here I am giving two thumbs up:

Sure, the prep was not a walk in the park. But it was not that bad. The colonoscopy itself? Heck I slept through all of it. Did it hurt? Not in the least. Was it embarrassing? Naw. (Yours is not the first nor the last rear end they will see and trust me, they don’t care at all what yours looks like).
I should point out that for some people, the prep really is miserable. For some, the sedation is not as effective as they would like. The procedure can be uncomfortable for some people, even painful. And as I mentioned above, for some (thankfully not too many) there are complications. So your experience may not be just like mine.
But I find that most people, even those who worried about it in advance, the colonoscopy turned out to be much less unpleasant that they imagined.
So if you are over 50 and have not done this yet: my parting advice is to pick one of these tests and DO IT. So many illnesses that afflict us can’t be prevented. This is not one of them.
David
Drop me a comment below if you want. And subscribe by e-mail if you like what you see. I promise, no spam or junk mail!
Getting to – and maintaining – a healthy weight
It is practically an expectation in health and wellness forums to talk about weight loss after the first of the year. New Year’s resolutions being all the rage in January. Perhaps you plan to lose a few pounds this year?
For me, it’s always around the middle where I put on a few pounds. You know, the little beer belly. The muffin top. The love handles. Begone, all of ye!
I was doing so well last fall, eating right, exercising more and so forth. Then winter in Minnesota hit. Now it gets dark at 4:30 in the afternoon. The perpetual ice slick on the sidewalks turn running or walking outside into a potentially bone-shattering experience. I mean, literally, bone-shattering as in broken hips and wrists. It has been so cold outside that your teeth hurt the minute you leave the house.
So I tend to hibernate a bit. Evenings on the couch reading next to a warm fire, although evoking images of Norman Rockwell, are not the way to shed pounds. Especially if I’m eating unhealthy foods all evening and maybe having a glass of wine with my chocolates. Wow that is starting to sound good: warm fire, wine chocolates, a good book . . . ah, but I digress. I’m supposed to be talking about diet and exercise here.
Reminds me of a post I did about the challenges of staying active in northern climates. Check it out here.
To show you the depth of my dedication to the cause of fitness, I included a recent photo of me above. Yup, that’s me all right.
Healthy life choices
So we talked weight loss and healthy livin’ on the show this week.
 To help me out, I invited a repeat guest to last Sunday’s Healthy Matters broadcast. Joining me on the radio show was Natalie Ikeman, who is a Physician Assistant HCMC’s Golden Valley Clinic. She runs “The Great Slim Down” weight loss program which you can check out here.
To help me out, I invited a repeat guest to last Sunday’s Healthy Matters broadcast. Joining me on the radio show was Natalie Ikeman, who is a Physician Assistant HCMC’s Golden Valley Clinic. She runs “The Great Slim Down” weight loss program which you can check out here.
If you missed the show, you can to the podcast by clicking the “Play” arrow here: ![]()
Tips for losing weight and keeping it off
Natalie gave us some great tips from her work with patients trying to lose weight. I’ll review some of them here.
Make goals.
With her patients, Natalie meets monthly to set goals. The good news is that they don’t have to be huge undertakings. The goals can be small changes in your daily lifestyle which you continually adjust, a process which Natalie refers to as “turning up the dial” on your goals.
Just a few examples of achievable goals are:
- Stress management tactics
- Better food choices
- Portion control when eating
- Finding time for daily movement, like taking small walks on your lunch hour
Nothing big, nothing huge, just small changes to your daily routine.
People who are successful at weight loss have some common characteristics:
Natalie’s patients in the Great Slim Down have lost an average of about 16 pounds. That is not only impressive but it is a sustainable amount of loss. She points out a few characteristics of these patients:
- They keep a daily record of their food intake. The simple act of recording what you eat – whether on paper or using one of the many apps for your mobile device – makes a person aware and less likely to fool themselves into thinking they are eating healthier than they really are. People usually eat more calories than they realize!
- They are active often in their daily lives. They find a way to move throughout the day.
- They are striving to meet their own goals, not goals set by someone else.
- They hold themselves accountable by sticking with it.
Pop (soda for those of you not from Minnesota) is not a healthy choice.
The sugar in soft drinks has virtually no nutritional value, and in fact, it probably leads to weight gain. For more on that, see my previous blog post, “Just a spoonful of sugar . . . is really not good for you.”
After Natalie and I suggested that we ought to avoid so much sugary soft drinks, a few listeners asked if diet pop is healthier. In a word, no. Although diet soft drinks are probably better than sugary drinks, they also contain ingredients that lack much nutritional value. Maybe stick to water!
So how about water?
For years, decades really, people have been taught to drink more water. Most of us probably remember the “8 glasses a day” advice. That is, in fact, what I told patients for years. But the reality is that there is not a lot of scientific evidence that otherwise healthy people need to drink more water than they already do. In other words, if you are thirsty you get a drink and if you are not, you don’t.

Photo: Jean Fortunet
So that’s it? Is that all there is to the water story – that it doesn’t matter?
Well, maybe not so fast. . . as we talked about on the radio program, there are some studies from this past year that suggest that there really is a benefit to drinking more water. One study found that more water was associated with less obesity. You can read about that one here. Another study found that drinking more water made people consume fewer calories, – check out this article about that one from the Atlantic.
I should caution that no single study can be used to definitely prove anything. Truth with a capital “T” is hard to come by in medical science! So whenever I refer you to studies like these, I do so to get you thinking about your own situation and not to imply that one study is proof of anything. Replication is the key in scientific studies (the findings of one study must be confirmed with separate studies).
But the water studies are at least thought-provoking. It makes sense to me that if you are focusing your liquid intake on water, you will be less likely to drink soft drinks and fruit juices that are loaded with calories and sugar. That has to be a good thing.
As Natalie said on the show, none of us should be “drinking our meals.” Amen to that.
Move more
One half of the healthy equation is Eat Less. The other half is Move More. But how? Most of us are not about to lace up our running shoes and hit the pavement for a long run. Most of us can’t get to the gym for a run on the treadmill or an exercise class. If you can do those things – great!
But lots of us have physical limitations that prevent vigorous work outs. And gym memberships ain’t cheap! So what can we do?
Let’s turn to Natalie again. As a companion to “The Great Slim Down” program, she has produced a series of short videos to give you ideas for exercise that may be right for you. Some are low intensity, others more vigorous. Some require standing and moving while others can be done by people from a seated position.
Here’s an example of one of Natalie’s videos:
To see the rest of them, go to the HCMC YouTube channel. If the link doesn’t work, simply search online for “HCMC YouTube channel” and click Playlists. You’ll find them there.
Housework is good for you
Listen to the show podcast (the player is above in this post). We talked about housework as a form of exercise. And you know what? It works. One listener to the show moved nearly 10,000 steps in one day simply doing housework. I complained that now I really have no excuse not to vacuum the house. Rats.
The Great Slim Down
I’ll close with one last word about the Great Slim Down. If you are in the Minneapolis area and struggling to lose some weight, maybe you should see Natalie. Simply call 612-873-6963 or check out the Golden Valley Clinic site here. No better time than now!
Thanks for reading. Hope you are all having a good day, a good week, a good winter where ever you are!
David
Butterflies and bacteria: thoughts on a healthy planet
 My family just returned from a pilgrimage of sorts. Having returned from a journey to witness one of nature’s miracles – and picking up a bit of a health problem myself – I’m feeling all butterfly-ish.
My family just returned from a pilgrimage of sorts. Having returned from a journey to witness one of nature’s miracles – and picking up a bit of a health problem myself – I’m feeling all butterfly-ish.
Please read on for my story and some thoughts about health, both the human, the insect, and the planetary kind.
(Except where noted, all photos are © David Hilden. Amazing what you can do with a camera phone) read more…