 See that brave patient in the picture? Yup, that’s me, just minutes from getting my colonoscopy at HCMC last year. I’ve been meaning to do a post about that experience and now seems as good a time as any. What with turmoil in the country and all, what could be better than to re-live the day somebody put a 5-foot long tube inside me to have a peek?
See that brave patient in the picture? Yup, that’s me, just minutes from getting my colonoscopy at HCMC last year. I’ve been meaning to do a post about that experience and now seems as good a time as any. What with turmoil in the country and all, what could be better than to re-live the day somebody put a 5-foot long tube inside me to have a peek?
It must be on lots of minds if last week’s radio broadcast was any indication. The phone and text and Twitter (@DrDavidHilden) lines were full of questions about colon cancer and how to avoid it.
Here’s the podcast of that show for you to listen to if you missed it (Healthy Matters show #420 – 1/22/2017)
I like to have a little fun with most medical topics, and I gotta say that if there ever was a medical topic worthy of humor, it has to be getting a colonoscopy. I mean, really, think about it. It has all the ingredients of a comedy routine:
- Gross part of the human anatomy. Check.
- Flushing out the entire contents of your intestines. Check.
- Baring your rear end to complete strangers while lying curled up on your side wishing you were literally anyplace else at that moment. Check.
- Complete surrender of any sense of dignity you had walking in the door. Check.
- Passing gas all day when it is over. Check.
What could be more fun?
But colorectal cancer really is no joke. In this post, I hope to accomplish three things:
- Convince you that getting screened for colorectal cancer makes sense.
- Introduce you to the various ways you can get screened.
- Allay any anxiety you may have over the whole subject.
Colorectal cancer: the bad news
In all seriousness, getting a screening test for colon cancer is among the most effective things you can do for your health. In fact, amid all the unpleasantries people endure in an effort to stay healthy, this one ranks way up there in importance. So let me repeat, getting screened for colon cancer is important and potentially lifesaving.
Check out the sobering news on colorectal cancer:
- It is common. Colorectal cancer is the 3rd most common cancer in men and women (skin cancers excluded).
- It can be deadly. Colorectal cancer is the second most common cause of cancer death in men (behind lung cancer), and the third most common cause of cancer death in women (behind lung and breast cancer).
- It is potentially treatable (and dare I say?), curable. Check this fact out – for those whose colorectal cancer is caught early, fully 90% will likely still be alive in 5 years. But for those with advanced cancer, only 15% will still be alive in 5 years.
A quick plug for some of the best medical information on the Internet. It comes from the Centers for Disease Control. For more on colon cancer from the CDC, click here.
It is largely because of that last bullet point that you should get screened for colorectal cancer. There is a dramatic difference in your chances of survival if you can only catch the cancer early on. That is true for most cancers, but it is especially true with this one.
This is a good time to point you toward the American Cancer Society’s Cancer Statistics Center. If you are curious about colorectal or any other cancer statistics, it is a great site to check out. You can sort the stats by your state of residence or type of cancer. It’s cool.
Ways to get screened
Hopefully I’ve convinced you of the importance of getting screened. Or maybe you didn’t need convincing in the first place! Let’s turn now to the various ways you can get the job done.
What you may not know is there are several ways to get your colon checked out. The one we all know and love is the colonoscopy but you may not know that it is not the only way to go. That surprises some people when I tell them that. There is a misconception floating around that the “best” way to go is the colonoscopy and that all the other methods are inferior. Not so, not so. It is the test of choice for many people (it is what I did) but it isn’t for everybody. And if the thought of an invasive procedure leads you to proscratinate forever in getting it, you are not getting the benefit of the test anyway.
As a wise person once said, “The best test for colon cancer screening is the one that the patient will actually do.”
So let’s look at the various tests you can consider:
FOBT and FIT tests
These are the tests in which you submit a little tiny stool sample and the test looks for blood in your stool that you can’t even see (hence the word “occult”). They are similar in that you usually can collect the sample at home, they are not invasive, and they are pretty good at finding hidden blood. They work under the principle that cancers and the pre-cancerous polyps in the colon tend to bleed.
FOBT stands for Fecal Occult Blood Test and sometimes has a little “g” in front of it (g = guaiac, so it looks like gFOBT). It’s the older one of the two and we’re seeing it used quite a bit less today. I think it will fade into oblivion . . . in favor of . . . FIT testing.
FIT stands for Fecal Immunochemical Test (sometimes written iFOBT with the little “i” = immunochemical). It is newer and uses a fancier approach to detecting blood proteins. It has the same advantages as the gFOBT but it has additional advantages over gFOBT in that it is probably more accurate and no dietary restrictions are needed prior to doing the test. Here’s a bit more on the FIT test.
Both of these stool tests need to be done every year. And if they find blood in your stool, you may need a colonoscopy after all! But they are a good choice for many people.
FIT-DNA
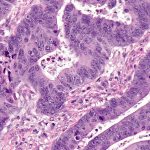
Photo: Nephron via Wikimedia Commons
This is the newest of the bunch. It works in a similar way to the FIT test above, but rather than look for blood, it looks for abnormal DNA in your stool. In other words, it is looking for the genetic “fingerprint” of cancer cells. Pretty cool, high-tech stuff here! The picture at left, though not of the DNA itself, is a biopsy specimen showing colon cancer cells. They are the angry looking cells throughout this piece of tissue.
This test needs to be done every three years but the data is not too certain on this yet since it is so new. It also may not be covered by your insurance. It is really promising though! We will be seeing a lot more of this one in the future, I think.
Flexible sigmoidoscopy
I’m not seeing too much of this method lately. It is sort of like a “mini-colonoscopy” in that a camera on a flexible tube is inserted into the colon. It doesn’t require the extensive colon flush, doesn’t need as much sedation, and complication rates are lower. Since it only looks at the lower part of the colon, however, it can miss any cancers that are higher up.
This test needs to be done every 5 years and lots of people get the stool tests in addition to it.
Colonoscopy
This is the one most of us think about. A specially trained doctor (a gastroenterologist – basically a really talented person with an inexplicable tolerance for looking at the nether regions of people) inserts a long-flexible camera into your intestines, all the way to the point where your large intestine (your “colon”) begins. Which is about 5 feet up there. Believe me, they are able to get a good look and simply see with their own eyes if you have a lesion (cancer or polyp). The advantage is that if they see something bad, they can either remove it entirely (like a polyp) or take a biopsy (to see if it is a cancer).
Cool picture time. Here’s a normal intestine as seen by your gastroenterologist (this one is actually in the rectum):

Photo: Melvil via Wikimedia Commons
Here’s an intestine with a polyp (don’t know if it is the pre-cancerous kind or not, but that’s why we take them out!)
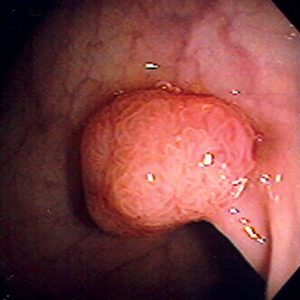
The other advantage is that for most people, colonoscopy only needs to be done every 10 years, perhaps every 5 years if they see something concerning.
But there are disadvantages to the colonoscopy. There is a small, but real, risk of perforation, which is where the colon wall gets a hole in it. And this is bad. Remember, your colon is full of bacteria and other unpleasantness. The outside of your colon (in your abdominal cavity) is sterile. You really don’t want the contents of your intestines to spew out into your belly. That can lead to a condition called peritonitis which can lead to sepsis which can be very serious.
Fortunately, this is a rare complication (estimates range from 1 in 500 all the way down to 1 in 6000). And although big perforations usually require surgery right away, many small perforations can heal themselves.
Virtual colonoscopy
I feel like I should mention this one (technically called CT colonography). It uses x-rays (a CT scan) to look at the colon non-invasively. Super tempting to go this route as it eliminates the invasiveness and thus the risk of colonoscopy. But I don’t see too many people getting the virtual test done. After all, it does expose you to radiation (albeit not a whole lot), and if it finds something abnormal, you still have to get the colonoscopy anyway.
My colonoscopy
I’ll end with my own story. I figure doctors who are counseling patients to get tested better be doing it for themselves, eh?
So I turned the magic age of 50 a while back and for most people, that is the age where all this colon talk gets real, real fast. I’m talking people at average risk. Others at higher risk (say your dad had cancer at an early age, for example) should do it sooner.
So I decided to go for it on a winter day last year. I saw my doctor (yup, I actually have a doctor that I see, though I have to admit it was turning 50 that prompted me to finally get a doctor of my own. Tsk-tsk, I know). He prescribed all the prep stuff which I faithfully did.
 Have you ever done the colon prep? Many of you remember getting such a large volume of the prep solution that you practically needed a grocery cart to get it home. You’d go to the pharmacy to pick it up, and they would push to you across the counter like a zillion gallons of the stuff in big jugs. You’d swear there was a mistake, that you were only getting the prep for one person not the whole family. But it was real. That was the way we used to do it (and still do for some people as it does actually work). You drank the solution the night before the colonoscopy until it came out the bottom end looking just like it did going in the top end – like clear water.
Have you ever done the colon prep? Many of you remember getting such a large volume of the prep solution that you practically needed a grocery cart to get it home. You’d go to the pharmacy to pick it up, and they would push to you across the counter like a zillion gallons of the stuff in big jugs. You’d swear there was a mistake, that you were only getting the prep for one person not the whole family. But it was real. That was the way we used to do it (and still do for some people as it does actually work). You drank the solution the night before the colonoscopy until it came out the bottom end looking just like it did going in the top end – like clear water.
My prep was of the newer kind. Instead of gallons of prep solution, I went the route where you pour an entire bottle of a laxative powder into a bottle of sports drinks and drink it down in a few sittings. Then you wait for the action to begin. And you spend most of the next 12-24 hours in the bathroom. This is a good time to get a supply of reading material and to tell your family to clear out of the place – for their own good.
Sometimes I think the people who devise these prep schemes are deranged.
So I did all that the night before my test. Then I show up for my colonoscopy to the GI Lab at HCMC, which is the hospital where I work. A couple points about that. First, why do they have to call it the GI Lab? Are they doing experiments in there? Second, it does take a bit of self-assurance to get your colonoscopy at your own workplace. I’m sitting there in a hospital gown with my rear end exposed for all the world to see when 2 or 3 people I see in the hallways all the time come in. Tough to maintain any sense of workplace decorum in that situation, I think.
So being the talker that I am, I try to make small talk with the nurse whom I know I will see a few hours later in the cafeteria line. He’s all professionalism, thankfully. And the doctor comes in, but I don’t make much eye contact with her, my backside being the side of interest, after all.
I assure the team that I will be watching my entire colonoscopy on the video monitor, just like Katie Couric did on live television a few years ago. And I really intended to watch because I was genuinely curious to take a gander at my own intestines from the inside out. That’s actually a pretty cool opportunity when you think about it. I thought I did a pretty good job staying awake. But then at one point I looked at the screen only to find out that the doctor was just finishing the whole procedure. She had done my entire colonoscopy and I dozed off for the whole of it!
I went home, had an uneventful day and made it to work the next day as good as new.
My point being: this was no big deal. To prove it, here I am giving two thumbs up:

Sure, the prep was not a walk in the park. But it was not that bad. The colonoscopy itself? Heck I slept through all of it. Did it hurt? Not in the least. Was it embarrassing? Naw. (Yours is not the first nor the last rear end they will see and trust me, they don’t care at all what yours looks like).
I should point out that for some people, the prep really is miserable. For some, the sedation is not as effective as they would like. The procedure can be uncomfortable for some people, even painful. And as I mentioned above, for some (thankfully not too many) there are complications. So your experience may not be just like mine.
But I find that most people, even those who worried about it in advance, the colonoscopy turned out to be much less unpleasant that they imagined.
So if you are over 50 and have not done this yet: my parting advice is to pick one of these tests and DO IT. So many illnesses that afflict us can’t be prevented. This is not one of them.
David
Drop me a comment below if you want. And subscribe by e-mail if you like what you see. I promise, no spam or junk mail!
