 Hi, everybody. I’m back with one of these “Quick tips” posts where I answer questions that were sent to me on a recent Healthy Matters radio broadcast. Regular listeners will know that I never can get to all of the questions, particularly those sent by text message, so I will try here to do some brief answers. I’ll keep it to just a few topics, and will do more posts in the near future.
Hi, everybody. I’m back with one of these “Quick tips” posts where I answer questions that were sent to me on a recent Healthy Matters radio broadcast. Regular listeners will know that I never can get to all of the questions, particularly those sent by text message, so I will try here to do some brief answers. I’ll keep it to just a few topics, and will do more posts in the near future.
Here are the topics in this post. Click the links to jump right to a specific topic.
- Influenza. How long are you contagious? What does it look like on a chest x-ray?
- ACE-inhibitors and high blood pressure.
- Kidney disease and protein in the urine.
- What is angina?
As always, I invite you to listen to the Healthy Matters broadcasts, either live or via podcast. Here are ways to listen:
- Live on News Radio 830 WCCO on your AM dial. Sunday mornings, 7:30 Central Time. You’d be surprised how far the WCCO signal reaches from our downtown Minneapolis studios.
- Live on WCCO.COM. Sunday mornings, 7:30 Central Time, from anywhere on Earth with Internet
- At your convenience, via podcast. Simply click on the “Listen to Podcasts” link right here on MyHealthyMatters.org or go directly to WCCO.COM on the “Audio” link and find Healthy Matters. You can listen directly online or you can download the podcast to your phone, tablet, or computer and listen anytime at your own convenience. Without commercials!
- Or just click the logo here:
Podcasts
Here we go with a Q&A from the listener lines from a recent broadcast (Healthy Matters show #472, January 21, 2018).
Q: If I have influenza A, how long am I contagious?
Photo by Edward A. “Doc” Rogers. From the Joseph R. Knowland collection at the Oakland History Room, Oakland Public Library.
A: This flu season is the worst we’ve seen in years, and it’s not over yet. It started earlier, seems to be lasting a good long time, and the strain of influenza (Type A, strain H3N2) is a nasty one. And the vaccine, though still the best defense we have, is not a great match this year. Flu hits you fast and hard – you are really sick with fever, muscle aches and cough. You are contagious for 24 hours before you have these symptoms and for up to a week after they go away. Children may be contagious even longer.
Here’s the latest statistics and graphs from the Minnesota Department of Health
Q: Pneumonia diagnosed but similar symptoms as the flu. What shows up on the x-ray?
A: Influenza and pneumonia can be hard to distinguish, especially since one of the more serious complications of flu infection is a secondary bacterial pneumonia infection (which usually sets in a week or two after the flu gets better). One way to tell them apart is a chest x-ray. On a chest x-ray, the typical pneumonia shows up as white opacities in the lungs. Influenza usually has no abnormal findings on a chest x-ray. Here’s some examples (chest x-rays are presented as if you are looking in a mirror or directly face-to-face with the patient, so right is left and left is right). The big blob on the left is the heart, for example.
Here’s an obvious opacity in the right lung. That’s pneumonia.
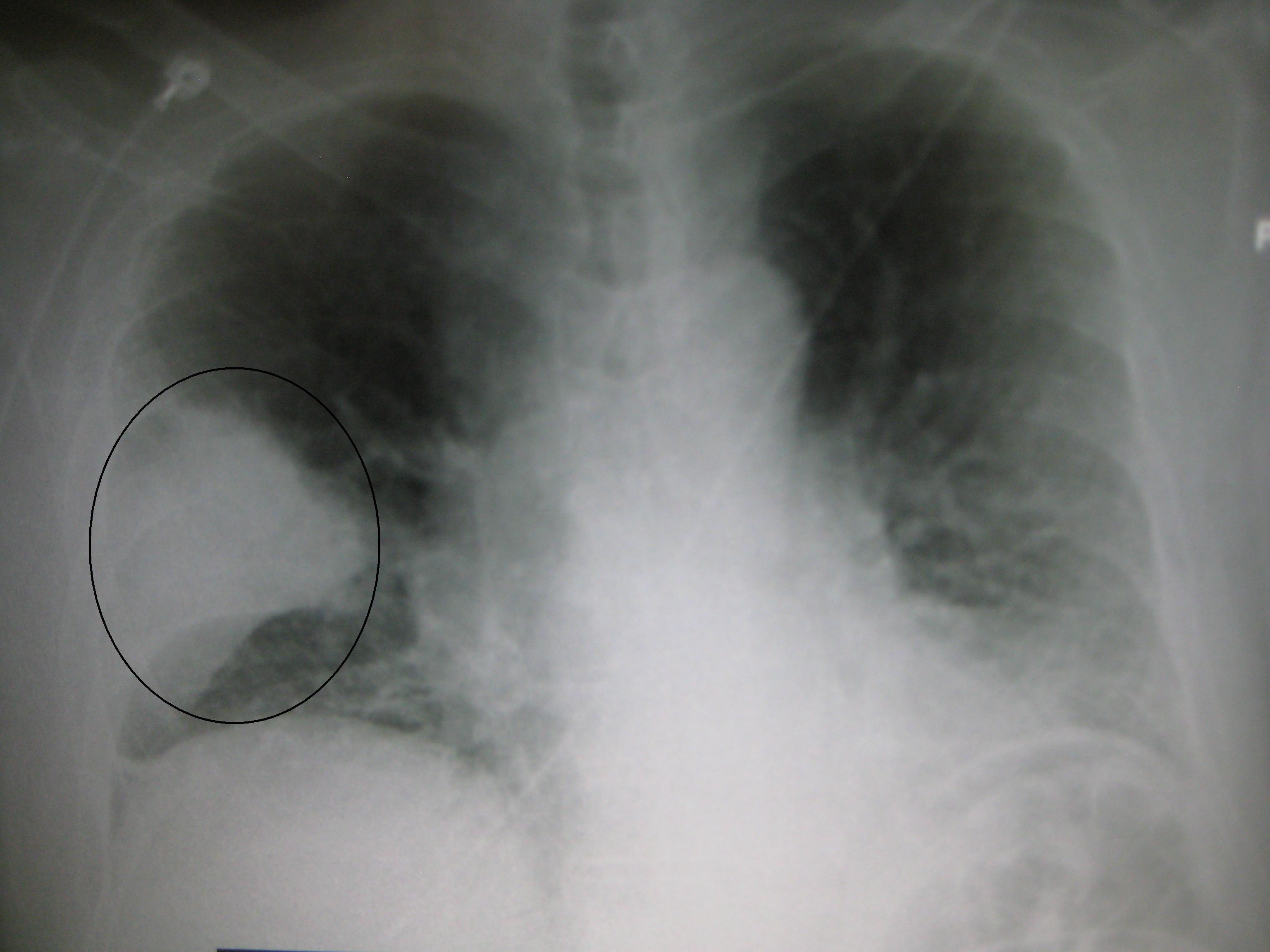
A clear and significant pneumonia in right lung
By James Heilman, MD, via Wikimedia Commons
Sometimes, pneumonia can be more subtle, like this one which is also in the right lung:
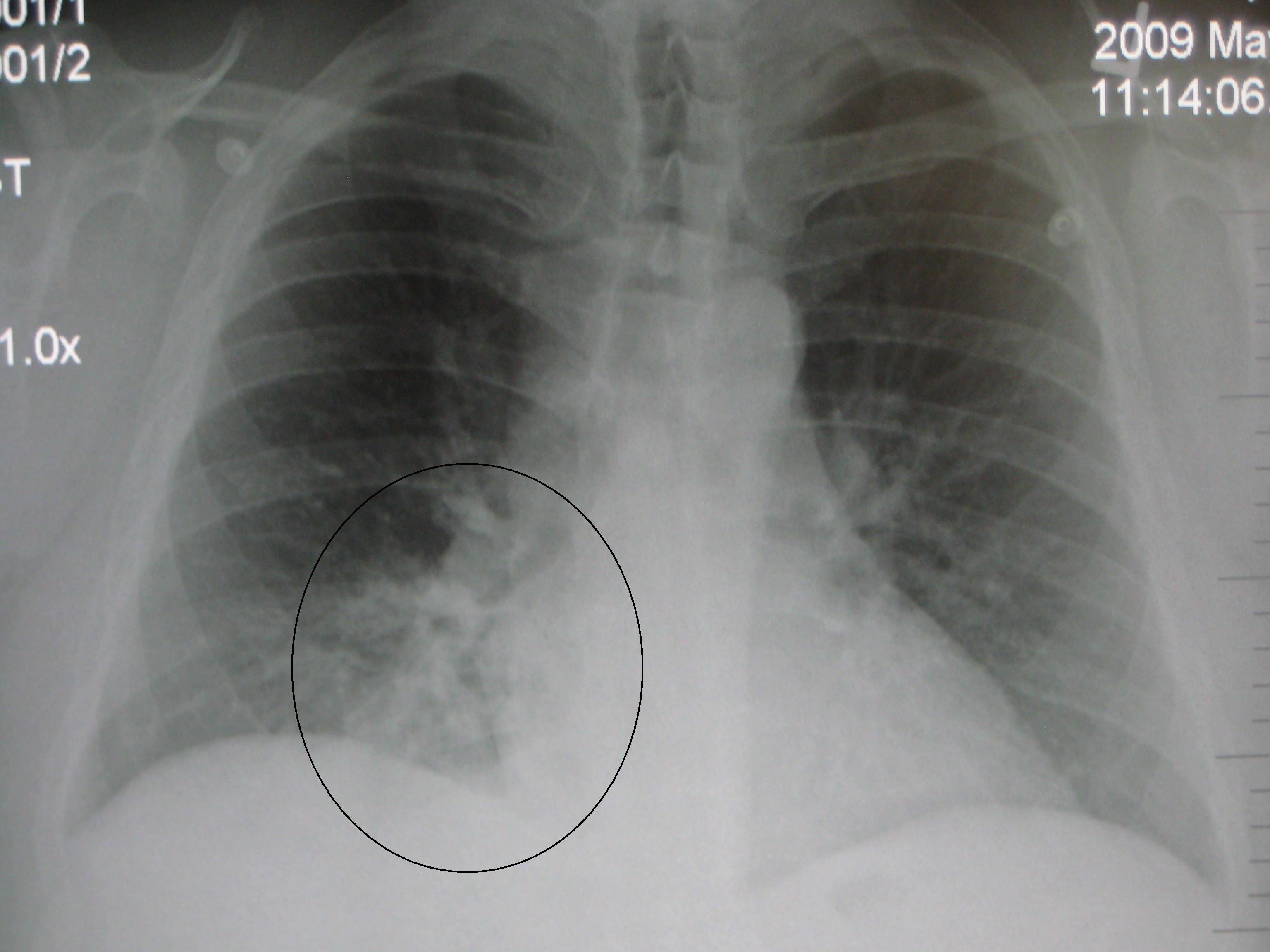
A more subtle pneumonia
By James Heilman, MD, via Wikimedia Commons
With influenza, there may be some minor and vague abnormalities, but usually the chest x-ray is normal, like this:

Normal chest x-ray.
By James Heilman, MD via Wikimedia Commons
Moving on from flu and pneumonia . . .
Q: I take lisinopril for blood pressure. I have a tickly cough that is annoying and pretty sure caused by the med. Is there a different option?
A: Yes! Lisinopril is one in a class of medications called angiotensin converting enzyme inhibitors, better known as ACE-inhibitors. They are usually very well tolerated with few side effects and they are quite effective at controlling blood pressure. That is why they are among the most prescribed blood pressure medications. But no medication is completely free of possible side effects, and with these meds, one of the more common side effects is a dry cough. Estimates are that between 1 in 50 all the way to 1 in 15 people may get a cough. Fortunately, the cough usually goes away when you stop the ACE-inhibitor. But there are lots of other blood pressure medications, including aldosterone receptor blockers (ARBs), calcium channel blockers (CCBs), diuretics (water pills), and even beta-blockers (though we usually use one of the others before a beta-blocker).
Q: What is microalbumin? I’m a diabetic, heart disease, mild Alzheimers and had a 3.55 reading.
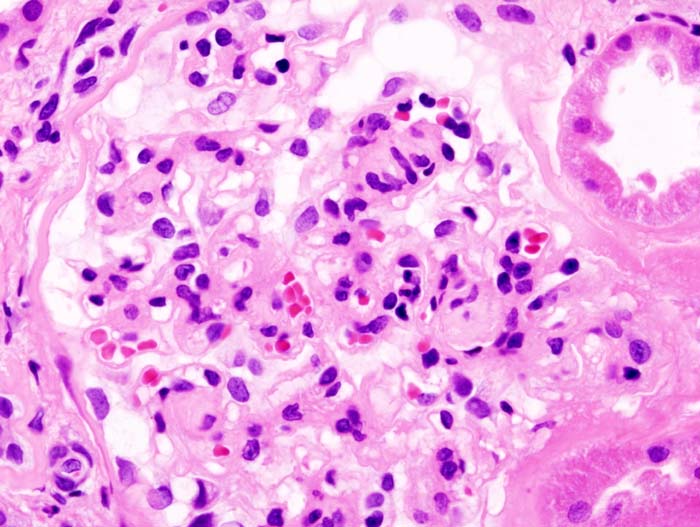
Glomerulus of a kidney biopsy in a person with diabetes
A: One of the very first signs of kidney disease is the presence of protein in the urine. Normally, urine has very little protein in it because protein is a relatively large molecule and the kidney keeps it in your body through millions of little filters, called nephrons, with each nephron containing a filtering structure called a glomerulus. (That is why the science of kidney disease is called nephrology). When the filtering mechanism gets sick, the proteins start to leak into the urine. We also know that it is good to catch kidney disease as early as possible since there are medications that can help protect the kidney from further damage. ACE-inhibitors are just such medications (see previous question). Albumin is just one of the proteins that can leak into the urine. So patients who have diabetes should regularly have their urine checked for microscopic amounts of albumin. Usually this “microalbumin” test is done once a year for people with diabetes. It catches kidney disease way before you would have any symptoms, so it’s an important part of overall diabetes health. We usually measure it as a ratio, and normal is a ratio <0.2. A ratio of 3.55 is way too high and represents “nephrotic range proteinura” – which is true kidney disease. I’m hoping the person posing this question is seeing a kidney doctor.
Q: What is angina? What causes it? What is treatment for it? Does it last for days, months, or years?
A: This question is actually from today’s show (February 4, 2018) but it is a good one with wide applicability.
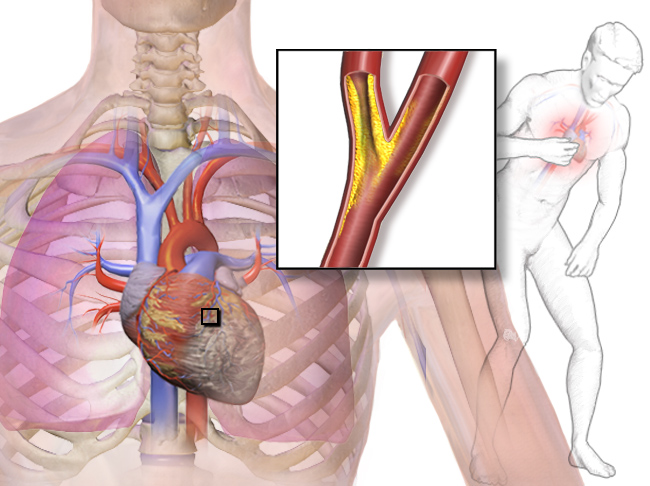
Blausen.com “Medical gallery of Blausen Medical 2014” via Wikimedia Commons
Angina pectoris is the full name and it refers to chest pain that results from partially blocked coronary arteries. It literally means “strangling of the chest” which is an awfully descriptive term. Most people pronounce it “ANN-gin-ah” (that’s how I say it) but others pronounce it “ann-GINE-ah” – whatever you prefer.
First a bit of anatomy. Being a muscle, your heart needs its own blood supply. The blood inside the heart can’t do this since it gets pumped to the far reaches of your body with each heartbeat. Rather, the heart gets its own blood supply from the coronary arteries which sit on the outside of the heart, not unlike a crown (coronary means crown). Here’s a picture:

By Patrick J. Lynch (1999), modified by Christian 2003 (Yale University – School of medicine) via Wikimedia Commons
Those coronary arteries can get partially blocked with time, diet, genetics, and simply aging. If they get completely blocked in an instant due to an unstable lesion in an artery, it is a heart attack. But the gradually “narrowing” of the arteries over many years leads to angina.
To answer the question specifically, angina typically occurs with exertion. This is because at rest, the heart doesn’t need as much blood and the narrowed arteries are sufficient to deliver what is needed. But with exertion, the heart demands much more blood, and those narrow arteries are not equal to the task. Chest pain, usually a pressure sensation, results.
How long does it last? Most angina lasts only a few minutes after the exertion stops. Doctors actually ask patients those two questions:
- Does it come on with exertion?
- Does it go away with rest?
If the answer is yes to both, it may be angina.
People can have angina many times during a day for many years. Or it can be relatively infrequent. It varies from person to person. The good news is that there are treatments. One good treatment is with the many anti-anginal medications that are effective. You can also get an angiogram and have a stent placed to relieve the blockage, though the scientific evidence for doing angiography and stenting for angina is not as great as you might think, though it is well-established that it is important for heart attacks.
There is a lot more about angina that I could say, but that’s a start. I’ll leave you with an important message:
Heart disease is still the #1 cause of death in the United States, and not all people have the typical symptoms of chest pain when having a heart attack. Some have nausea, some have arm and jaw pain, some have back pain, and so on. If you have chest pain or other symptoms that may be your heart, time is the worst enemy you have! Call 911 immediately and get taken by ambulance to a hospital where you can get immediate attention.

Look for more Quick Tips in future posts. Thanks to MyHealthyMatters readers and listeners for your questions!
Reporting to you just hours before Super Bowl LII, which is conveniently across the street from me. Fans are pouring in. It’s 3 degrees outside. The military choppers and flyovers are underway.
Skol, Vikings . . . . next year!
Best wishes to Eagles and Patriots fans!

I have the best view from HCMC!
